
Children wearing multifocal contact lenses had slower progression of their myopia, according to results from a clinical trial funded by the National Eye Institute, part of the National Institutes of Health. The findings support an option for controlling the condition, also called nearsightedness, which increases the risk of cataracts, glaucoma and retinal detachment later in life. Investigators of the Bifocal Lenses In Nearsighted Kids (BLINK) Study published the results August 11 in the Journal of the American Medical Association.
“It is especially good news to know that children as young as 7 achieved optimal visual acuity and got used to wearing multifocal lenses much the way they would a single vision contact lens. It’s not a problem to fit younger kids in contact lenses. It’s a safe practice,” said BLINK study chair, Jeffrey J. Walline, O.D., Ph.D., associate dean for research at the Ohio State University College of Optometry.
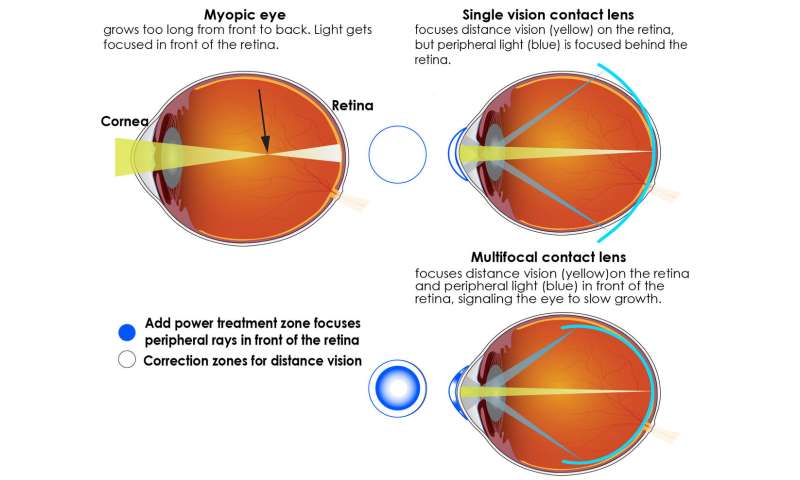
Myopia occurs when a child’s developing eyes grow too long from front to back. Instead of focusing images on the retina—the light-sensitive tissue in the back of the eye—images of distant objects are focused at a point in front of the retina. As a result, people with myopia have good near vision but poor distance vision.
Single vision prescription glasses and contact lenses are used to correct myopic vision but fail to treat the underlying problem. Multifocal contact lenses—typically used to improve near vision of people over the age of 40 years—correct myopic vision in children while simultaneously slowing myopia progression by slowing eye growth.
Shaped like a bullseye, the soft multifocal contact lenses have two basic portions for focusing light. The center portion of the lens corrects nearsightedness so that distance vision is clear, and it focuses light directly on the retina. The outer portion of the lens adds focusing power to bring the peripheral light rays into focus in front of the retina. Animal studies show that bringing light to focus in front of the retina cues the eye to slow growth. The higher the power added, the further in front of the retina it focuses peripheral light.
By comparison, single vision glasses and standard contact lenses focus peripheral light to a point behind the retina, which prompts the eye to keep growing.
The researchers examined whether high-add power contact lenses provided better slowing of myopia progression and eye growth than medium-add power contact lenses. They found that only the high-add power contact lenses produced meaningful slowing of eye growth.
In addition to multifocal lenses, other myopia control options include orthokeratology contact lenses, which are worn overnight to reshape the cornea, or low-dose atropine eye drops used at bedtime.
The U.S. Food and Drug Administration approved one lens for myopia control in November 2019, but multifocal contact lenses have been used off-label to slow myopia progression for many years.
Myopia has surged in prevalence over the past five decades. In 1971, 25% of Americans were myopic, compared to 33% in 2004. By 2050, the worldwide prevalence of myopia is projected to be 54%, and the prevalence of high myopia, the most severe form, is projected to increase to 10%. High myopia means that a person’s vision requires at least -5.00 diopters, the unit of focusing power correction required to optimize distance vision.
Reasons for the spike are unclear, but evidence suggests that near work, such as screen time, and shrinking outdoor time during early eye development are contributing factors. Genetic factors also play a role in one’s predisposition to become myopic.
There are no tests to identify which individuals with myopia will progress to high myopia, but the younger a child is affected, the more opportunity their myopia has to progress if there is no intervention to slow it.
Study participants were 287 myopic children, ages 7 to 11 years. At baseline, the children required -0.75 to -5.00 diopters of correction to achieve clear distance vision. The children were randomly assigned to wear single vision contact lenses or multifocal lenses, the outer lens of which were either high-add power (+2.50 diopters) or medium-add power (+1.50 diopters). They wore the lenses during the day as often as they could comfortably do so. All participants were seen at clinics at the Ohio State University, Columbus, or University of Houston.
After three years, children in the high-add multifocal contact lens group had the slowest progression of their myopia. Mean myopia progression, as measured by changes in the eye prescription required to correct distance vision, was -0.60 diopters for the high-add group, -0.89 diopters for the medium-add group, and -1.05 diopters for the single vision group.
The multifocal lenses also slowed eye growth. The three-year adjusted eye growth was .42 mm for the high add group, .58 mm for the medium add group, and .66 mm for the single vision group.
“Greater amounts of myopia and longer eyes are associated with increased prevalence of eye conditions that can lead to visual impairment. Our study shows that eye care practitioners should fit children with high-add power multifocal contact lenses in order to maximize myopia control and the slowing of eye growth,” said principal investigator, David A. Berntsen, O.D., Ph.D., associate professor and Golden-Golden professor of optometry at the University of Houston.. “Compared with single vision contact lenses, multifocal lenses slow myopia progression by about 43% over three years.”
“There is a clear benefit from multifocal lenses at three years, but further study is needed to determine the ideal duration for wearing the lenses. Researchers will need determine how permanent the prevention of myopia progression will be once children stop wearing the multifocal lenses,” said Lisa A. Jones-Jordan, Ph.D., principal investigator of the Data Coordinating Center at the Ohio State University. A follow-up study is underway to see if the benefits hold among children in this study when they go off treatment.
Source: Read Full Article